
Heart Defects
What you need to know
Endocarditis & Prevention | Heart ID Card
What is bacterial endocarditis?
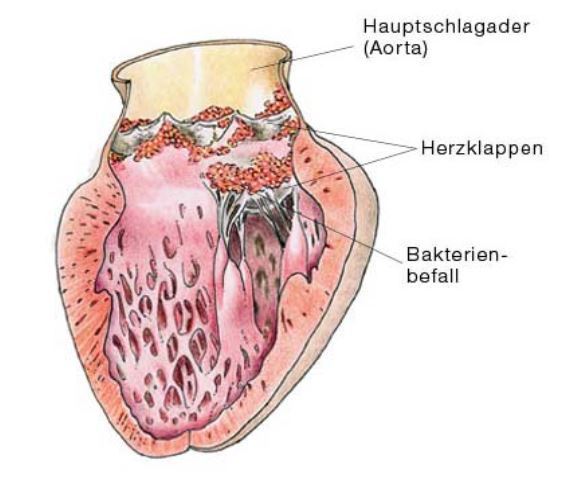
Under certain circumstances, bacteria can travel to the heart and colonise diseased, damaged or operated heart valves. There is a similar risk for patients with artificial or bioprosthetic heart valves. Patients with certain congenital heart defects may also be affected by bacterial colonisation. Treating endocarditis is a long and drawn-out process. Depending on the bacteria and the severity of the infection, a variety of different antibiotics are usually administered intravenously over a period of 4-6 weeks. In severe cases, the infection may destroy one or several valves, requiring emergency surgery. To avoid endocarditis, some patients with heart conditions will have to take antibiotics preventively in certain situations.
What is bacterial endocarditis prophylaxis?
During dental or surgical procedures, bacteria can find their way into the bloodstream (bacteremia). Once in the blood, the bacteria can adhere to and destroy the damaged heart valves. To prevent this from occurring (prophylaxis), antibiotics are administered whenever a bacteremia is anticipated.
Who requires endocarditis prophylaxis?
Patients with congenital heart defects (e.g. ventricular septal defect, open ductus arteriosus/Botallis, tetralogy of Fallot, patients with left-to-right shunts) need endocarditis prophylaxis, as they have a heightened risk of getting endocarditis. The same applies to all patients with operated, artificial or bioprosthetic heart valves or who have had bacterial endocarditis in the past.
Which interventions require endocarditis prophylaxis?
Prior to a surgical or dental procedure, the patient should ask whether endocarditis prophylaxis is required. Endocarditis prophylaxis is especially recommended for interventions in the mouth and throat (pharynx) and endoscopic examinations or surgical interventions in the upper airways (bronchoscopy, tonsil operation). Surgical interventions in the gastro-intestinal tract are likewise associated with an increased risk of bacteremia (gastroscopy, colonoscopy). Interventions in the genito-urinary tract (kidneys, genitals), where the urine is sterile, do not require prophylaxis.
Who decides whether endocarditis prophylaxis is necessary and how is it carried out?
Given the large number of indications and surgical interventions, deciding whether endocarditis prophylaxis is needed can often be difficult. All patients should be issued an “Endocarditis Prophylaxis ID Card” by their doctor. They should show the ID card to doctors/dentists in advance of any procedure that involves risk. In complex situations, the patient should consult a cardiac specialist/cardiologist.
An endocarditis prophylaxis is carried out by giving the patient antibiotics before and after the intervention. The Endocarditis Prophylaxis ID Cards contain exact details of the type of antibiotics and the duration of treatment required. These recommendations are based on the guidelines published by the European and American Society of Cardiology.
Hauptschlagader - Aorta
Herzklappen - Heart valves
Bakterienbefall - Bacterial colonisation



